Naturally, maintenance crews are seen as fixers, rebuilders, and restorers. However, poorly executed maintenance work can actually become the source of future problems.
And when things go wrong, they can go terribly wrong. In fact, EU OSHA states that around 10-15% of all fatal accidents are related to maintenance operations.
This article will examine some of these disasters, and the role that maintenance played in causing them. There are several themes behind these disasters: the safety program missing fundamental pieces, workers not following procedure, or safety plans lacking rigor and precision.
In selecting these case studies, we attempted to cover a variety of scenarios. All can be deemed “disasters” for various reasons, and there are not necessarily any events that should be thought of as “worse” than others. With that stated, let us start reviewing the case studies.
Guide to Moving from Reactive to Preventive Maintenance
Want to transition away from costly reactive maintenance but don't know where to start? This guide has everything you need to know.
Safety program missing fundamentals
With all of the advances in worker safety over the last 100 years, there are still countless facilities that are lacking basic adequate safety measures:
- Non-existent or inadequate Lock Out Tag Out program
- Non-existent or inadequate Management of Change (MOC) program
- Poor safety training and procedures
- Lack of adequate PPE
If you do not think that sounds particularly bad, here are some examples that might change your mind.
Disaster #1: Lack of an MOC program
In 2007, at the Valero McKee Refinery, a release of propane led to a massive fire. The damage was extensive – in excess of $50 million. Three employees and a contractor were injured.
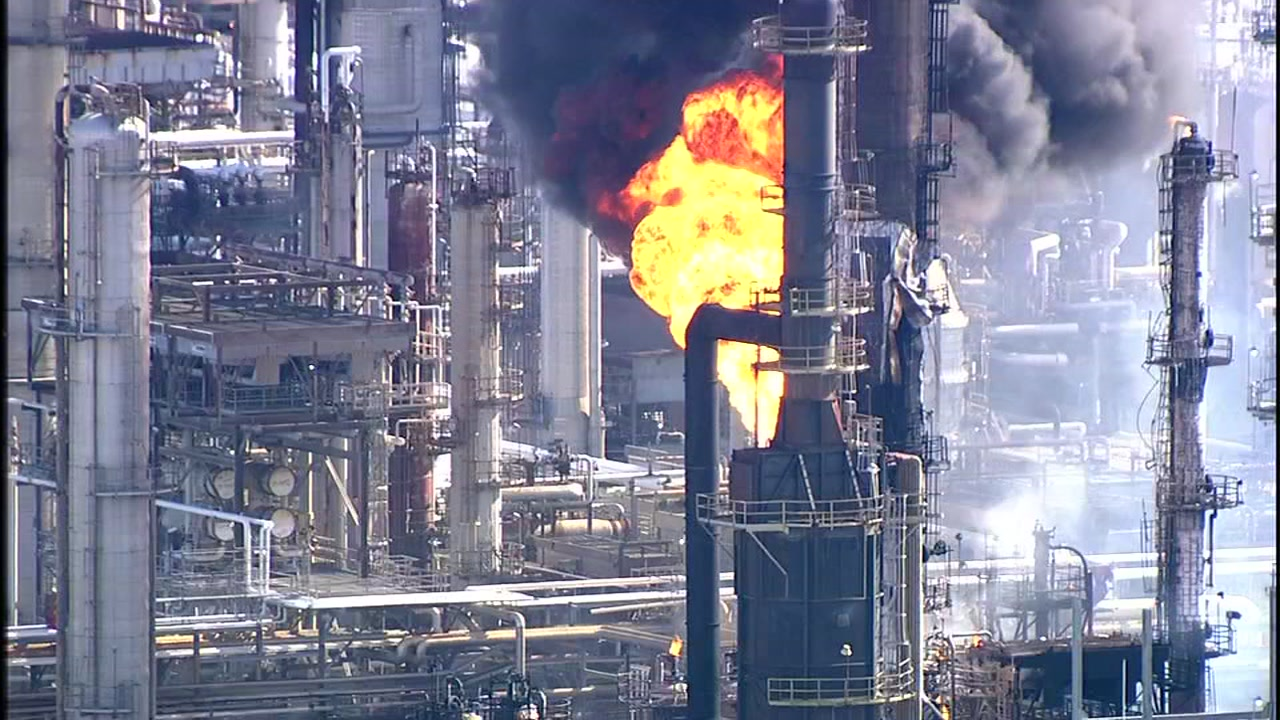
The source of this disaster was traced back to abandoned old equipment. A section of pipe that had not been used in 15 years was left attached to the process. Small amounts of water accumulated over the years and froze in low temperatures, which cracked the pipe. The crack gave an outlet for propane to escape and form a vapor cloud. The vapor ignited, starting an enormous fire disaster.
Valero never conducted a Management of Change process when it removed the piping from service in 1990. An MoC could have caught the risk of this event, or perhaps led to a plan to remove the piping. No maintenance or inspections were ever done on the piping after it was abandoned. Any of these fundamental measures could have prevented the fire.
Disaster #2: Not following LOTO procedure during maintenance
In an incident in 2019, an employee was servicing a baler. Blades were stuck into a bale and they needed removal. One maintenance worker started working on the issue. They failed to lock out and tag out the equipment they were working on. There was a shift turnover and the next crew took over the work, also without locking out the machine.
Then when a worker was assisting in the removal of material, the baler turned on. This worker lost their hand in the accident. The business had to pay a hefty fine to OSHA.
The reason for this incident is abundantly clear: if the baler had been properly locked out by anyone involved, it would have been impossible to power on. In an ideal scenario, everyone involved in the work would attach their personal lock to a lock box, adding layers of protection for each individual.
Disaster #3: Lack of adequate training and directions
In 2020 at Evergreen Packaging Paper Mill, a fire occurred during a shutdown maintenance activity on a pulp bleaching tank. The fire resulted in the deaths of two contract workers on site.

The pulp bleaching tank normally stored corrosive material, which affected tank areas. Though the tank was corrosion-resistant, it required periodic maintenance on the inside surfaces.
In this case, contractors were applying polyester resin and fiberglass to the inside of the tank. The resin was not hardening in normal time, and it was sliding down and accumulating at the bottom of the tank. The contractors tried several approaches that were not successful.
Ultimately they decided to bring a portable heat gun into the tank to aid in curing. This heat source was a dangerous addition to a flammable atmosphere, and it led to an ignition of the resin. The fire spread to a connected tank, where the flames and smoke overcame two contract workers.
One of the main causes of this incident was a lack of training for the contractors. They were unaware that a heat gun was a deadly addition to a flammable atmosphere inside a tank (the heat gun temperature exceeded the flash point of the flammable resin.) Furthermore, Evergreen failed to provide adequate training or clear directions to the contractors, and also failed to properly monitor the work.
Not following proper procedures
Many incidents arise from workers not following proper procedures. In some cases, the workers are trying to cut corners. In others, they are pressured to speed up their maintenance activities.
When certain steps are critical, there must be additional safeguards in place. These could be as basic as establishing maintenance approval forms, where every job has a checklist that must be verified by another person of authority.
Disaster #4: A common practice of breaking procedures
In a 2013 incident, a Virgin America employee was working on an aircraft engine. Because the approved lift trucks were unavailable, he decided to use a portable stepladder. This action went against the established procedure for the site.
The employee fell from the ladder, breaking several ribs and injuring his spine. He was hospitalized and underwent multiple surgeries. The employee later stated it was common practice to break the procedure.
There are countless examples mirroring this incident – where workers deviate from established written policies. The correction is not simply to tell employees to follow procedures. You have to find the root cause and address it (policy not understood, tools not easily available, etc.).
Disaster #5: Not enforcing established rules
An excavator laborer was working at a site using a pneumatic mole to dig out an area for maintenance. During the excavation, he struck an underground 11,000 Volt electric cable and was burned severely. He was hospitalized, where he later died.
How did this occur? When undergoing any excavations, it is critical that utility lines be checked beforehand – even if there is a belief that no danger exists. HSE states: “The site rules were not being enforced by the Principal Contractor despite high-risk work being undertaken.”
Undoubtedly the site had rules on utility line checks that were not followed, to dire ends.
Disaster # 6: Cutting corners due to time constraints
At a power generation facility in 2015, three workers were performing maintenance. Their job was replacing a transformer. They started by taking voltage readings on various spots on the transformer.
As they were working through the procedure they noticed a discrepancy in the expected readings. They stopped to take more readings and noticed a small arc in current. The supervising group told the maintenance technicians to work faster. They returned to the work, and as they continued, three were burned from arcing current. Two employees suffered from first-degree burns.
The cause for this incident is once again rooted in not following procedures. When the maintenance crews found abnormalities, they paused and tried to understand the situation. But their management pushed them to finish the job. Instead, they should have followed proper safety measures to determine the discrepancy and the arc source.
Maintenance execution lacking expertise and rigor
Many businesses make attempts to build a safety program, but ultimately fail because they do not follow through properly. This could be due to a lack of experience, resourcing, or knowledge.
It is vital to find help when there are deficiencies in expertise. As we will see in the next few examples, the consequences can be severe.
Disaster #7: Lack of quality control
In 2008, a two million gallon fertilizer storage tank collapsed at the Allied Terminals facility. The collapse resulted in flooding a containment dike, overflowing liquid fertilizer into the nearby residential neighborhood. The residents had to evacuate their homes for several days, and a specialist environmental firm had to be brought in to assist with the cleanup.

A welder and his assistant were working on the tank when it ruptured. They were exposed to large quantities of fertilizer, which severely injured them.
The cause of the tank collapse was attributed to an inadequate weld. Allied Terminals was relying on a contractor that did not weld to industry standards, and they did not have an inspector who could identify the deficiencies. The lack of collective expertise led to dire consequences.
Disaster #8: Poor maintenance management system and reporting
In 2010, an operator was transferring phosgene from a cylinder to a process vessel. While he was checking the weight of the cylinder, the hose ruptured. The operator was sprayed in the face with phosgene. Though he did not show immediate signs of acute sickness, the operator later began feeling weak and was admitted to the hospital. His condition rapidly deteriorated and he passed away.
Among the causes of the hose failure were:
- An ineffective maintenance management system. The system did not have internal authorizations, or create automatic hose change-out tasks based on set intervals. Thus no one was keeping track of hose usage to replace them before catastrophic failure.
- Weak emergency notification process. The site did not have emergency radio channels or phone numbers established. Because of this, it took too much time for the site to realize what had happened and to decontaminate the exposed worker.
- Substandard hazard-reporting program. There wasn’t a formal process for employees to report hazards onsite. So even though some were aware of the problems with old hoses, they could not report these to management in a proper way.
Even though no tool can compensate for the absence of important procedures, a good CMMS solution would help alleviate most of the problems stated above. With a centralized database to schedule and organize maintenance work, as well as track all maintenance history and failure causes, it is very unlikely that an organization would experience such a communication breakdown and be unaware of issues with deteriorating equipment.
Disaster #9: Incorrect screw set installation
In July 2020, the ship Atlantic Huron, a 736-foot bulk carrier, lost its propulsion control. The ship was attempting to slow down, but it was instead speeding up. This led to the ship barreling into a pier, causing $2.2 million in damages.
How did this happen? The answer is quite technical, yet surprising: it was due to an
incorrect installation of a single set screw on the propeller machinery that controlled pitch. This ship had a pitch propeller, where the blades could be rotated to determine the speed and direction of the vessel.
The set screw on the pitch propeller had not been installed using thread-locking fluid. Over time, the screw slowly backed out. This set off a chain of failures which resulted in the ship moving forward instead of backward.
The remedy for this incident is not so simple. The set screw problem is very hard to detect. At the very least, the ship should have had a procedure to respond to the pitch propeller malfunctioning.
Preventive maintenance is an investment, not a cost center
In putting this list together, it was especially distressing knowing that all of these events were preventable.
Take this as a warning sign. Review your safety program with respect to maintenance. When you find gaps, set out to correct them. With enough attention to safety policies and maintenance procedures, you can keep your site, equipment, and workers safe.
If you need help with scheduling and tracking preventive maintenance work, Limble CMMS has your back. Maintenance calendar, parts and vendor management, compliance audit reports, predictive maintenance, and so much more – all available without breaking the bank. Start a 30-day free trial today and never look back.